History: A 79 year-old woman presented with a two year history of a slow-growing oral cavity mass between the buccal mucosa and cheek, near the lip commissure. Her past medical history was unremarkable.
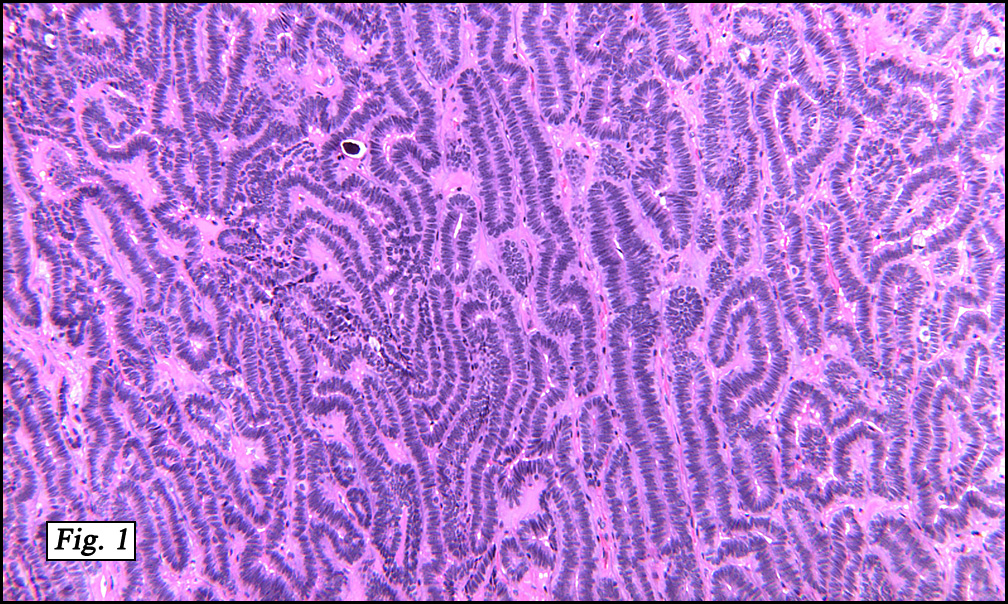
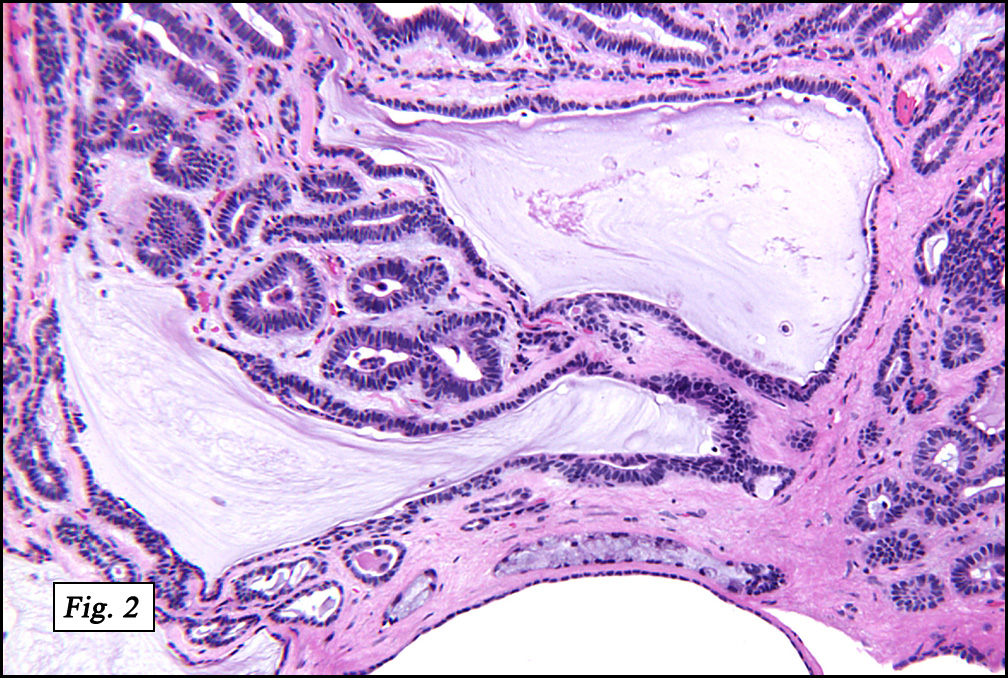
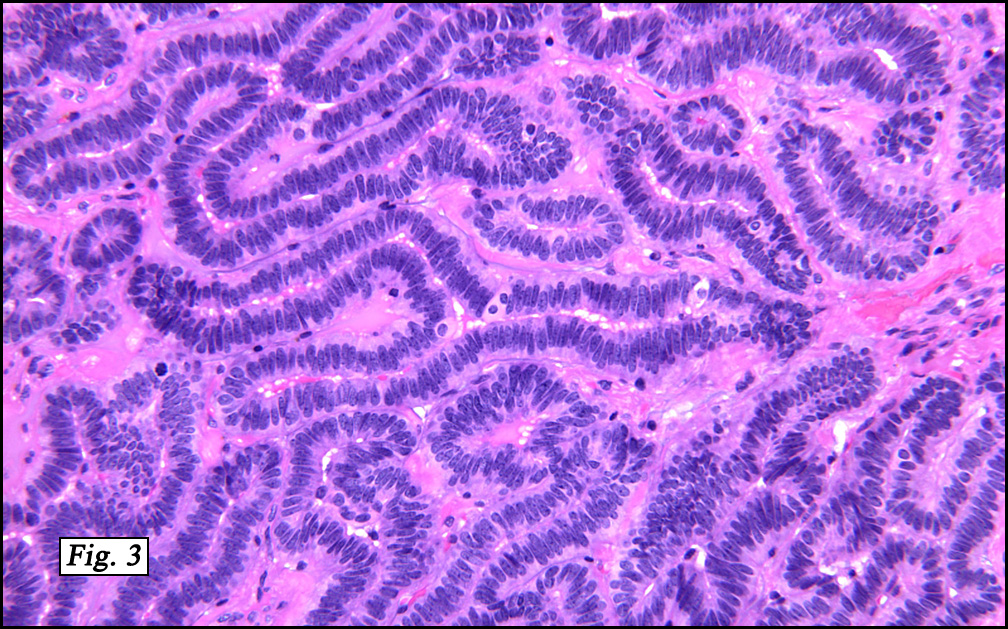
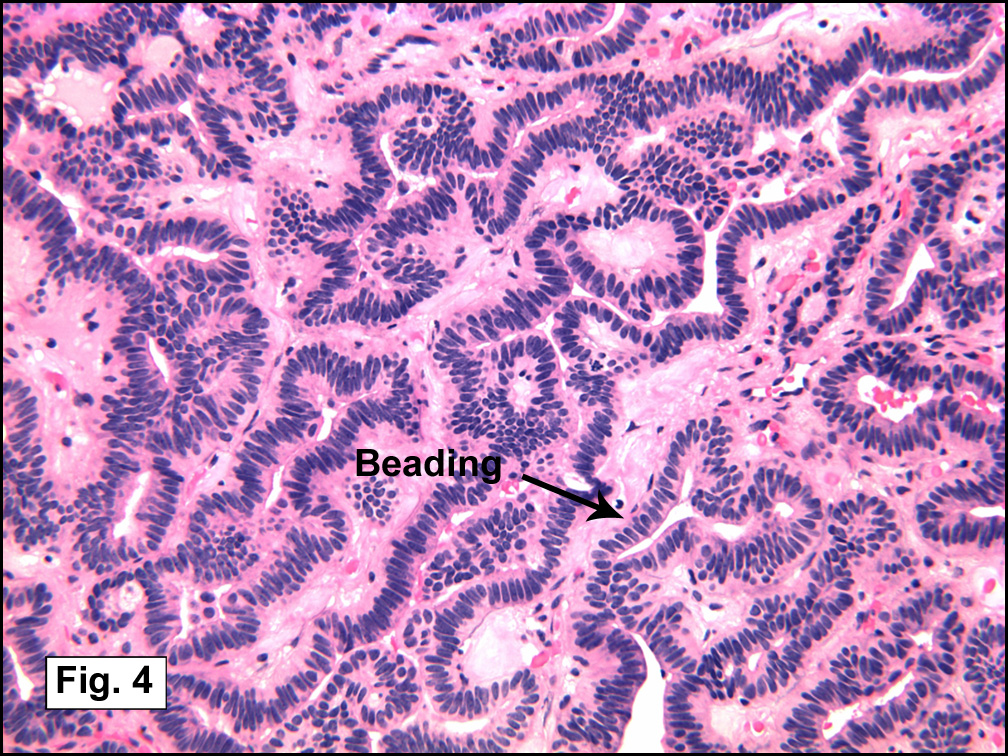
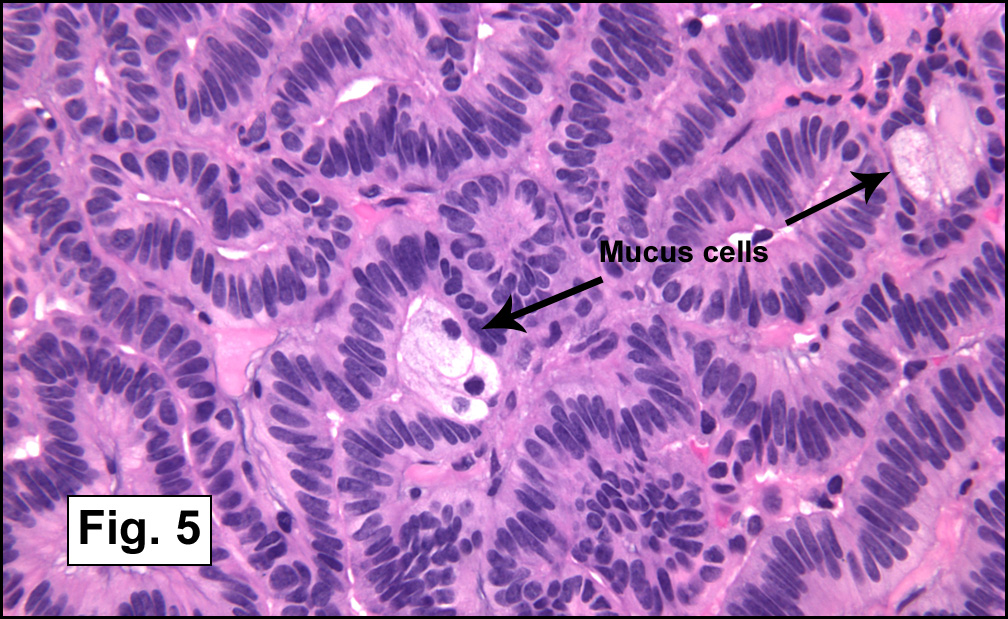
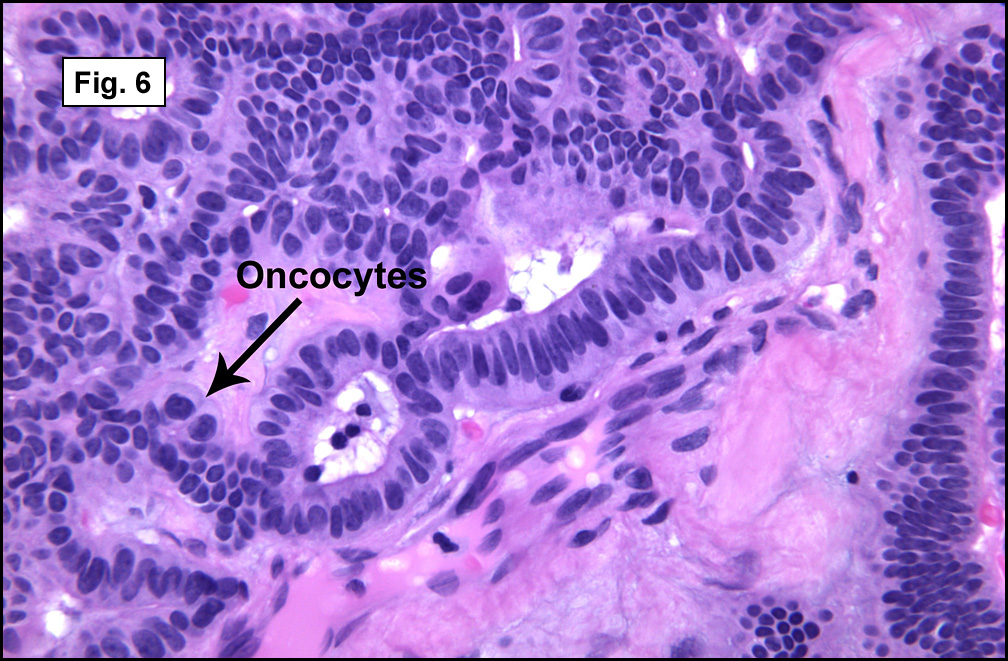
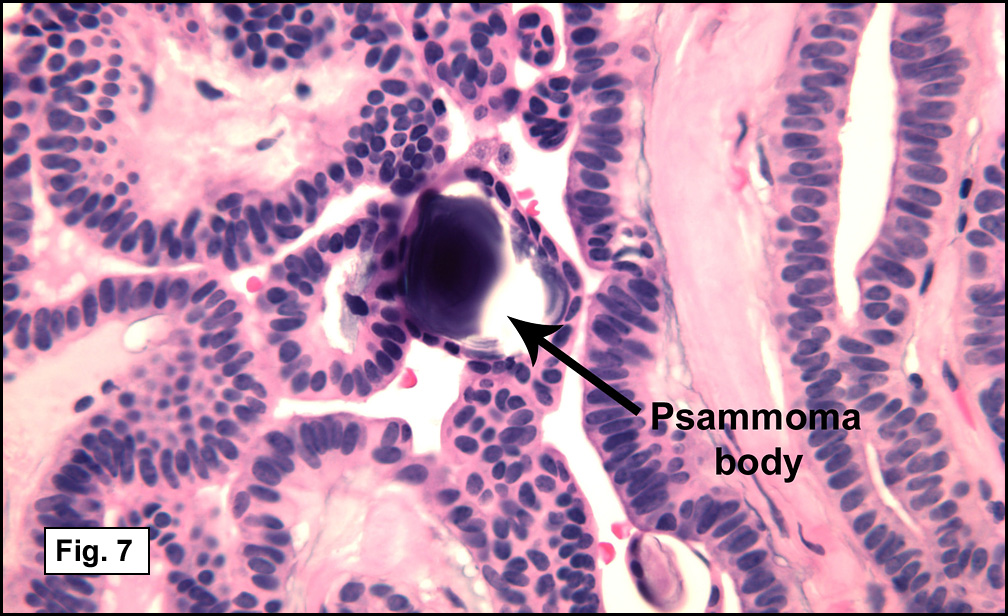
Sections showed a well-circumscribed, nodular, thinly encapsulated epithelial neoplasm. The tumor was predominantly composed of a solid proliferation of cytologically bland cuboidal to columnar basaloid cells with dark nuclei and scant eosinophilic cytoplasm (Fig. 1). Microcyst formation was focally present (Fig. 2), sometimes associated with fine papillae. The periphery showed the mucous pattern of minor salivary glands. Lesional cells were usually bilayered in branching/anastomosing cords (i.e. trabecular pattern) (Fig. 3) The cords sometimes separated and rejoined repeatedly, creating a “beaded†appearance (Fig. 4). Scattered foci of mucous cells (Fig. 5), oncocytic cells (Fig. 6), and squamous metaplastic cells were seen. Psammoma bodies were scattered throughout the tumor (Fig. 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Canalicular Adenoma of Minor Salivary Gland Originâ€
Melissa Skaugset MSIV, Mia Perez MD, Donald Chase MD
Department of Pathology and Human Anatomy,
Loma Linda University and Medical Center
California Tumor Tissue Registry, Loma Linda, California
Discussion: Canalicular adenoma (CanA) is a benign epithelial neoplasm of the salivary glands that, by the WHO definition, is composed of columnar epithelial cells arranged in thin, anastomosing cords often with a beaded pattern. The stroma is characteristically paucicellular and highly vascular. They are benign neoplasms, only rarely recurring after local excision. Synonyms include:
• Basal cell adenoma, canalicular type
• Monomorphic adenoma, canalicular type
• Adenomatosis of minor salivary gland
Canalicular adenomas most commonly affect the minor salivary glands. The majority arise in the upper lip (70-90%) where they are the second most common salivary gland tumor after pleomorphic adenoma. Their next most common site is buccal mucosa. Only rarely have they been reported in the parotid gland or palate.
CanAs are rare before the fifth decade of life, and have a peak in the seventh decade. No clear gender prevalence has been shown. They usually present as slow growing, painless small mass(es). They are freely mobile, frequently multinodular, and usually are less than 2 centimeters in greatest diameter (mean 1.7cm). They are generally slow growing, and have been reported to have been present for up to 15 years. The majority present as a solitary mass, but up to 22% are reportedly multifocal and/or multiple (Daley, 1984). Grossly, they are well demarcated and frequently encapsulated. The tumor is usually solid and homogenous, but may have cystic inclusions filled with mucoid material.
CanAs were long thought to be a subclass of basal cell adenoma due to its phenotypic similarity, but is now thought to be a distinct entity. It derives its name from the double rows of cuboidal to columnar epithelium that separate and rejoin to form small duct-like structures or canaliculi. The pattern of separation and rejoining evokes the image of beads on a rosary, leading to descriptions of “beading†or “rosary beadsâ€. The epithelium may be cuboidal or columnar and is usually without significant cellular atypia or pleomorphism. The stroma is loose, highly vascular, and usually of low cellularity. Cyst formation is common.
Unlike other salivary gland tumors which may show multiple growth patterns, canalicular adenomas tend to have a predictable patterns. But they may vary in cellular density and amount of cyst formation, and the degree of encapsulation. The diagnosis may be made without special stains, although recognized positive markers include keratin, vimentin and S100. GFAP may be focally positive. The tumors do not react to anti-SMA.
The differential diagnosis includes sebaceous cyst, lipoma, nasolabial cyst, and more commonly, salivary gland tumors that have a “basaloid†pattern, i.e. basal cell adenoma and adenoid cystic carcinoma. Distinguishing basal cell adenoma from canalicular adenoma has limited clinical significance apart from the potential of canalicular adenomas for multifocality. Distinguishing this entity from adenoid cystic carcinoma is much more important. The double rows of columnar cells and canaliculi that typify canalicular adenomas are not seen in adenoid cystic carcinoma, although the cribriform and tubular patterns of the latter can be confused with this pattern. Nuclear irregularity and atypia are present in adenoid cystic carcinoma, but not in an adenoma. Vascularity of the stroma of canalicular adenomas is absent in adenoid cystic carcinoma. Dense collagen may surround cell nests in adenoid cystic carcinoma but is typically present only in the capsule of canalicular adenoma.
Suggested reading:
Barnes L, Eveson JW, Reichart P, Sidransky D. WHO Classification of Tumours: Pathology and Genetics of Head and Neck Tumours, 2005 Ed. IARC Press, International Agency for Research on Cancer, 2005. p 267.
Peel RL, Barnes L. Surgical Pathology of the Head and Neck. Marcel Dekker, New York, 2001. pp 663-670.
Ellis GL, Auclair PL, Rosai J. AFIP Atlas of Tumor Pathology: Tumors of the Salivary Glands. American Registry of Pathology, Armed Forces Institute of Pathology, Washington D.C., 1995. pp95-103.
Kratochvi F, Ellis GL, Auclair P, Gnepp D. Surgical Pathology of the Salivary Glands. W.B. Saunders Company, Philadelphia, 1991. pp 202-212.