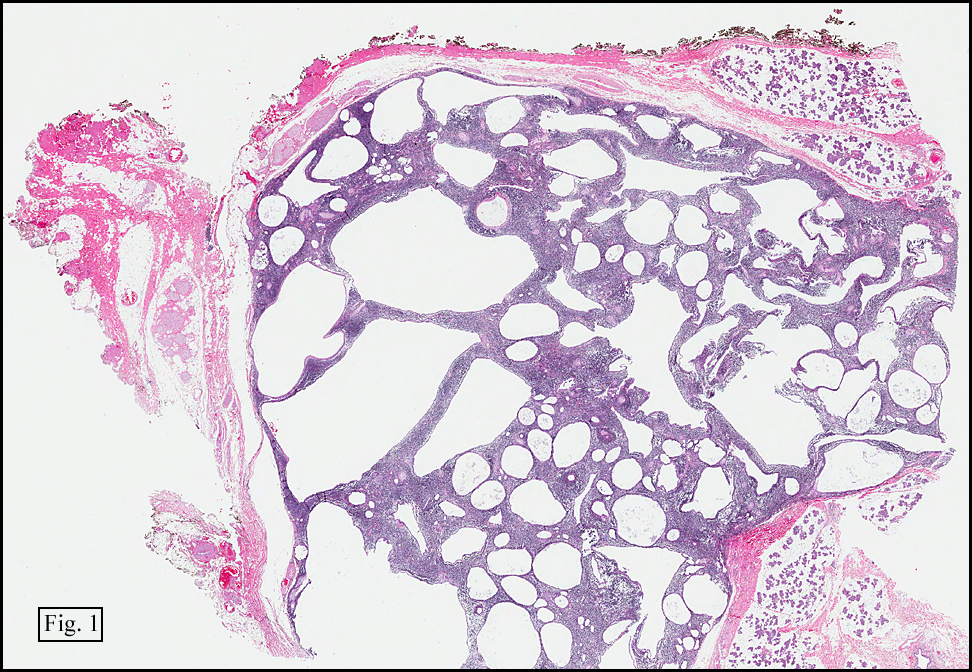
History: A 74 y/o man presented with a two year history of a left-sided facial mass. A CT scan identified a 4.0 cm mass in the parotid gland. Following a FNAB which showed only “reactive†lymphoid elements, a superficial parotidectomy found a well-circumscribed grey-tan cystic mass containing cheesy, grumous material.
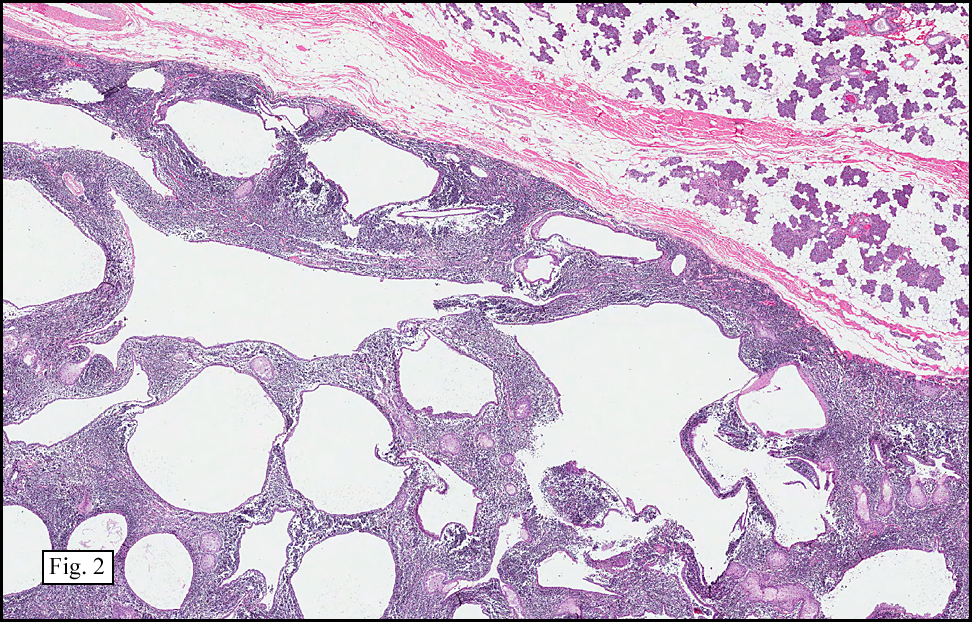
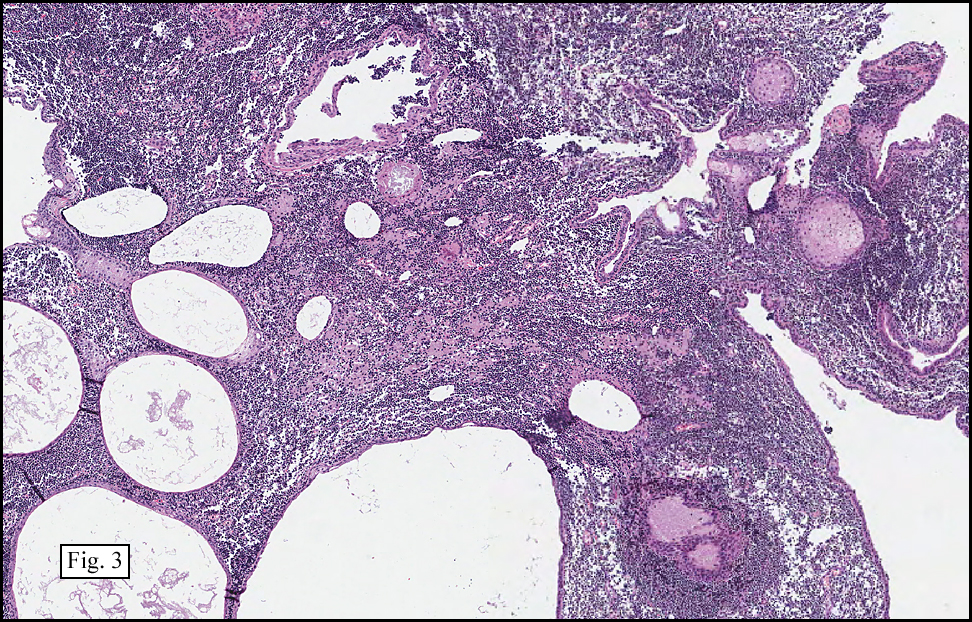
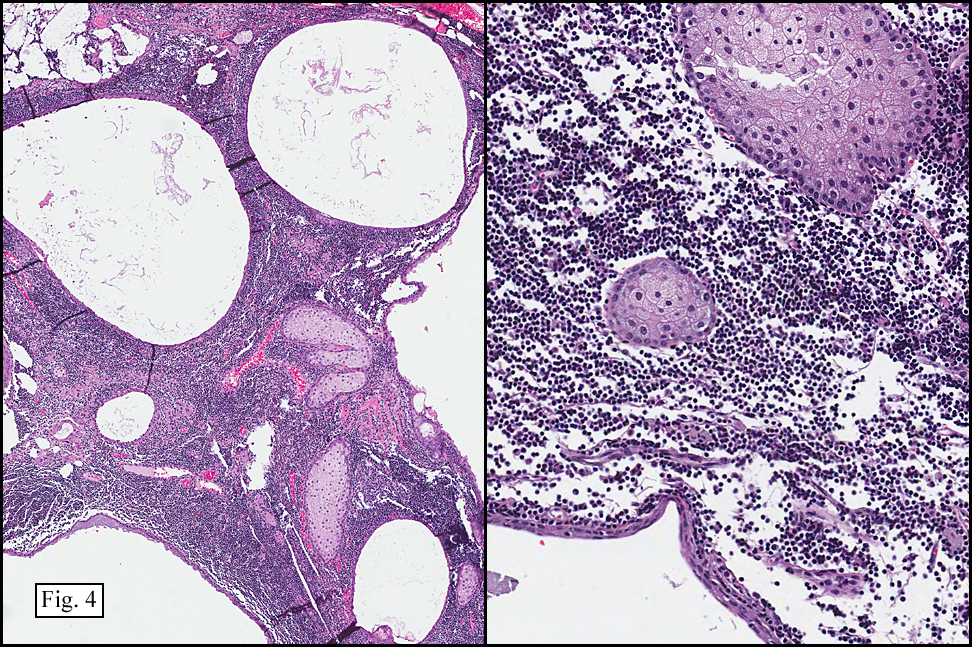
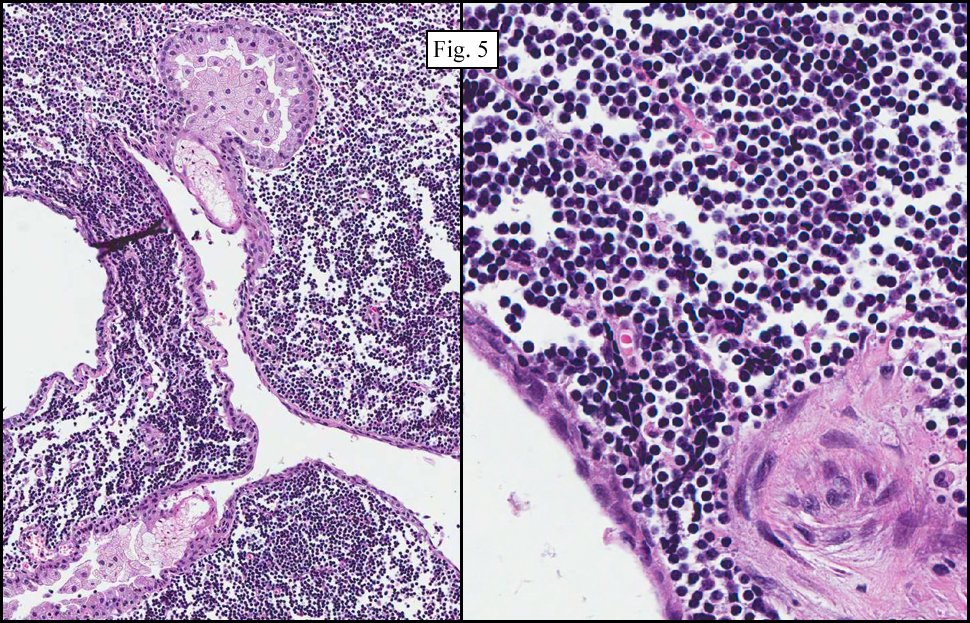
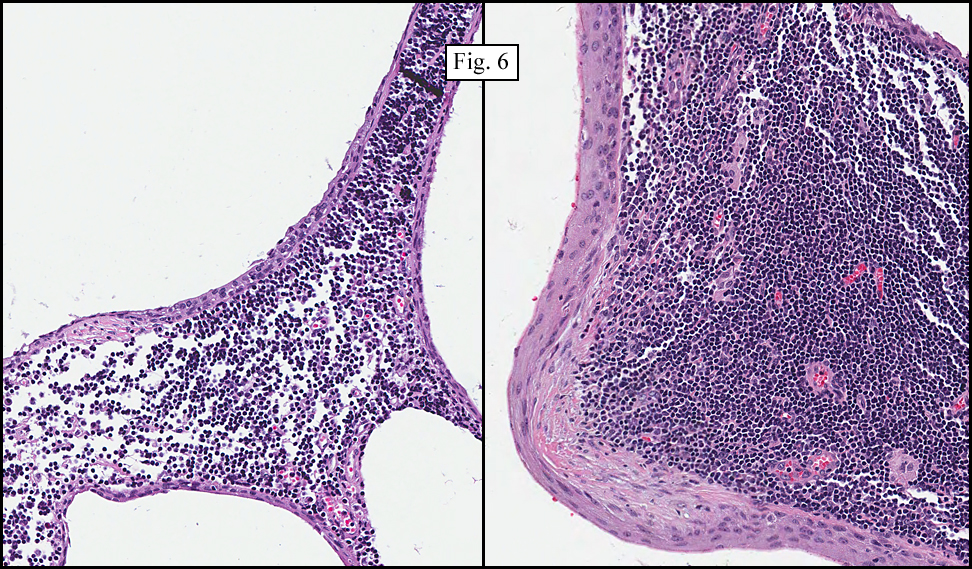
Microscopically the tissue had a “pushing margin†abutting the parotid gland (Fig. 1, 2). It consisted of solid epithelial nests and small cysts or duct-like structures with focal sebaceous elements (Fig. 3). The background was of lymphocytes, without atypia (Fig. 4). In addition to the sebaceous elements, were scattered squamous pearls, and a yst lining of simple squamous to low cuboidal epithelium (Fig. 5,6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Sebaceous Lymphadenomaâ€
Christina Martin MSIV, Donald R. Chase MD
Department of Pathology, Loma Linda University and Medical Center, Loma Linda California Tumor Tissue Registry, Loma Linda, California
Discussion: Sebaceous lymphadenoma (SL) is a rare benign epithelial tumor making up less than 0.1% of all salivary gland neoplasms. Most often occurring between the ages of 50-80, these tumors present as a progressively enlarging, painless mass. They are most commonly found in the parotid gland, but have also been reported in the oral region and the anterior midline of the neck. Some cases have been associated with a simultaneous Warthin tumor or primary squamous cell carcinoma.
Fine needle aspiration usually demonstrates aggregates of sebaceous cells with foamy cytoplasm and central crenated nuclei, as well as less mature squamoid forms with dense cytoplasm and rounded nuclei. A background of small mature lymphocytes may also be seen.
The excised specimen is usually described as solid to multicystic, and pinkish-grey to white or yellow. Sebum-filled spaces are sometimes present. Capsules are usually well-developed, but may be partially or completely absent. When absent, the periphery is still well-circumscribed, reflective of expansive compression of surrounding tissues.
The microscopic appearance of SL is usually of epithelial nests with peripheral basaloid cells maturing inwardly into sebaceous cells. Duct-like structures and small to medium sized cysts lined with squamous, cuboidal, columnar, and sebaceous cells are also seen. Many of the lumens contain secretions, and occasionally there are keratin-filled cysts. Oncocytic changes may also be present. The prominent lymphoid stroma is uniformly dense, but does not usually invade the epithelial elements. Lymphoid follicles may be absent or numerous, with mantle zones ranging from ill-defined to well-formed.
Immunohistochemical features include positive cytokeratin and epithelial membrane markers in the epithelial elements. S-100 and smooth muscle actin are generally negative. The lymphoid component has similar staining properties of a reactive lymph node.
The nature of the lymphoid tissue in sebaceous lymphadenoma is controversial, paralleling the controversy surrounding the lymphoid component of Warthin tumors. One theory is that the tumors arise from ectopic salivary gland tissue entrapped in lymph nodes during embryogenesis. Another suggests that the lymphoid component represents a secondary reactive response to epithelial proliferation (tumor-associated lymphoid proliferation) as seen in various other parotid gland tumors. The latter explanation is favored by current WHO and AFIP publications.
Treatment of this lesion is local excision. Recurrence is rare.
Some important entities to distinguish from Sebaceous Lymphadenoma include:
Lymphadenomas are identical tumors but lack sebaceous differentiation.
Mucoepidermoid carcinoma with tumor-associated lymphoid proliferation has a more haphazard distribution of cysts and ducts, and more variation in their size and shape than sebaceous lymphadenoma. Other distinguishing features pointing towards mucoepidermoid carcinoma include papillary growth and extensive, poorly organized intraluminal proliferation of the lining epithelium of the cysts, as well as the presence of clear and intermediate cells.
Sebaceous Adenocarcinoma forms irregular islands and narrow cords of tumor cells, but unlike sebaceous lymphadenoma, the cells infiltrate surrounding connective tissue and salivary gland parenchyma. The peripheries are infiltrative, not “pushing.â€
Metastatic adenocarcinoma or squamous cell carcinoma can be a concern when seeing epithelial islands within a lymphoid stroma, however in sebaceous lymphadenoma they are morphologically bland and do not infiltrate surrounding tissue.
Suggested Reading:
Thompson’s: Head and Neck Pathology: a Volume in the Series Foundations in Diagnostic Pathology. Editors Thompson LDR, Goldblum JR. Elsevier, Inc. pp 312-15, 2006.
AFIP Atlas of Tumor Pathology: Tumors of the Salivary Glands. Editors Ellis GL, Auclair PL, pp 136-141, 2008
Sebaceous lymphadenoma of parotid gland in a child. Sun G, Hu Q, Huang X, Tang E. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Feb; 107 (2): 253-5.
Sebaceous lymphadenoma of the parotid gland. Majeed M, Murray B, Hume W, MakuraZ. Dentomaxillofac Radiol. 2008 Jul:37(5):300-4.
Lymphadenoma of parotid gland: Two additional cases and a literature review. Dardick I, Thomas MJ. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008 Apr;105(4):491-4.
Sebaceous lymphadenoma of salivary gland: a case report and a review of the literature. Maffini F, Fasani R, Petrella D, Maiorano E, Bruschini R, Pelosi G, Viale G. Acta Otorhinolaryngol Ital. 2007 Jun;27(3);147-50.
Sebaceous lymphadenoma of the parotid gland: report of two cases and review of the literature. Hayashi D, Tysome JR, Boyei E, Gluckman P, Barbaccia C. Acta Otorhinolaryngol Ital. 2007 Jun;27(3):144-6. Review.
Unilocular cystic sebaceous lymphadenoma: a rare tumor. Chandrasekar T, Ramani P, Anuja N, Karthikeyan R, Abhilash PR, Narayan V, Giri VV. Ann R Coll Surg Engl. 2007 May;89(4):1-3.
Sebaceous lymphadenoma identified by fine needle aspiration biopsy: a case report. Banich J, Reyes CV, Bier-Laning C. Acta Cytol. 2007 Mar-Apr;51(2):211-3.