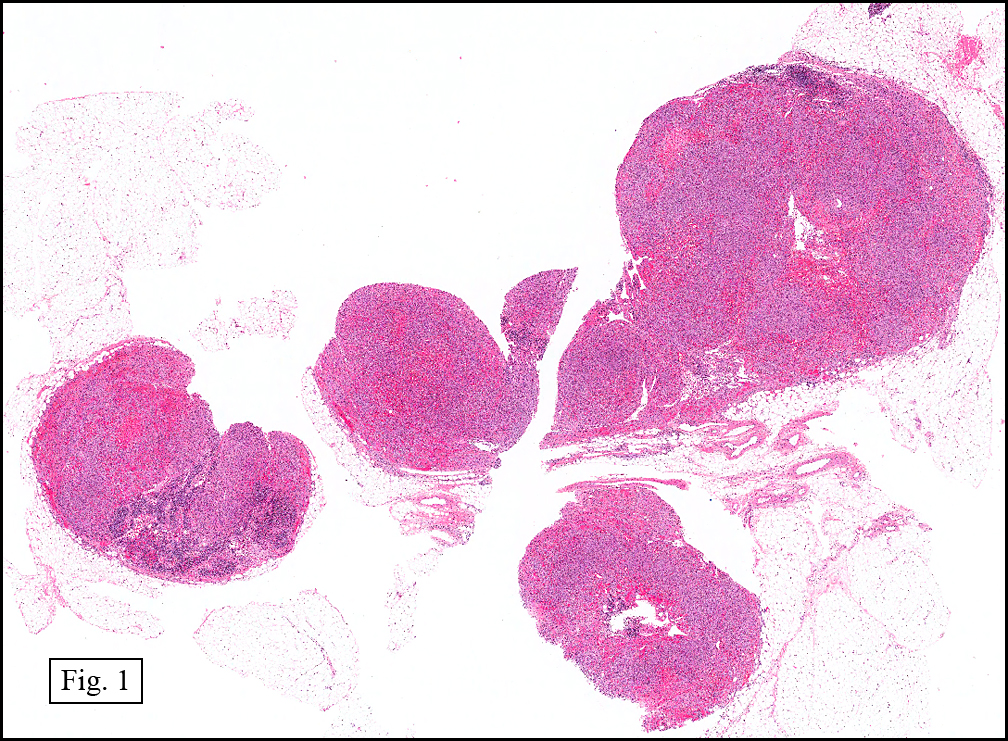
History: A 31 y/o physician with a retroviral disease and associated immunodeficiency was found to have cervical lymphadenopathy. He had a chronic cough, but sputum had been negative for mycobacterium and PCP. There was no evidence of fungal or acid fast bacilli. No skin lesions were found and there was no history of previous neoplasia. Excisional lymph node biopsy was performed. The specimen was received in multiple fragments (Fig. 1)
{kind=link}
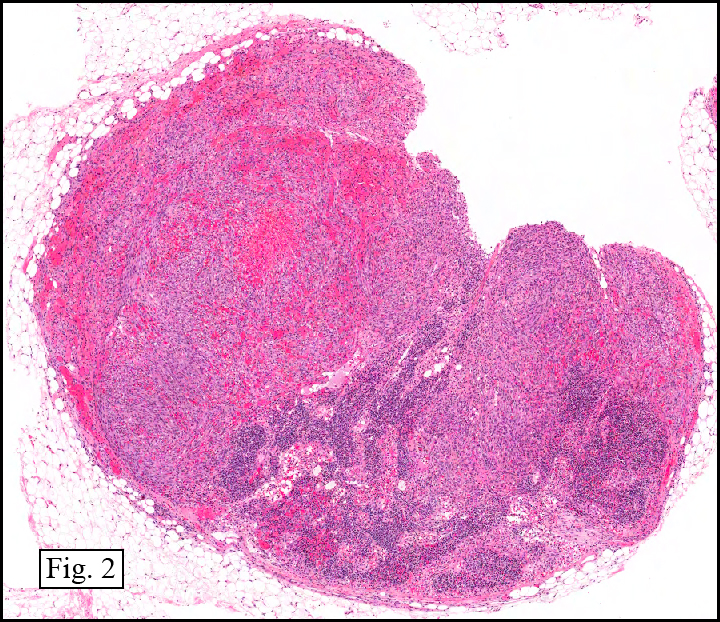
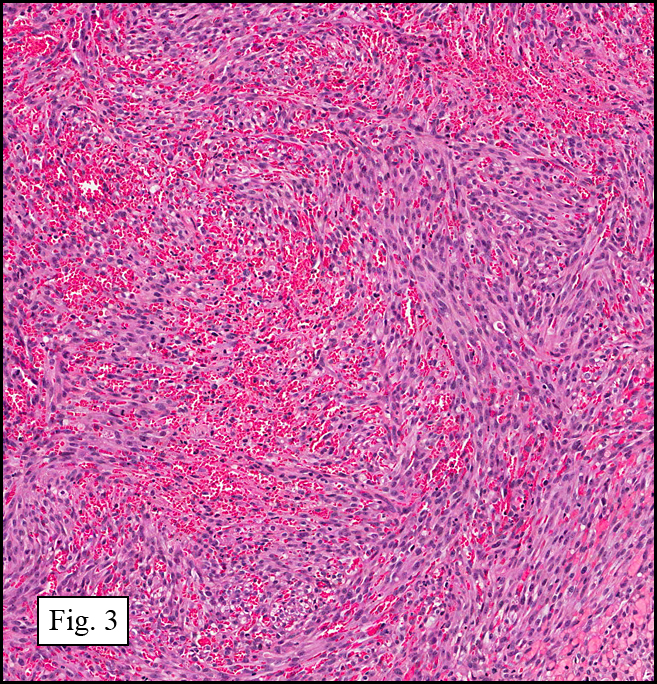
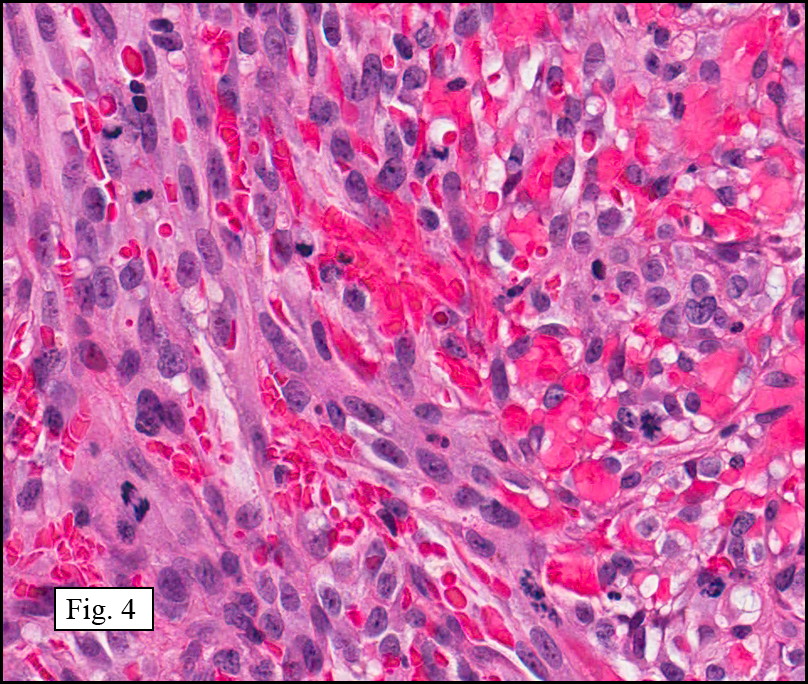
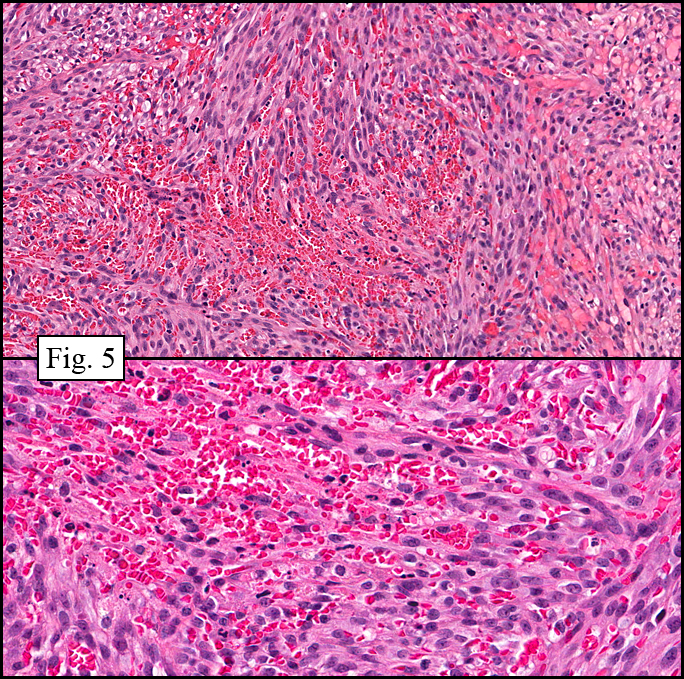
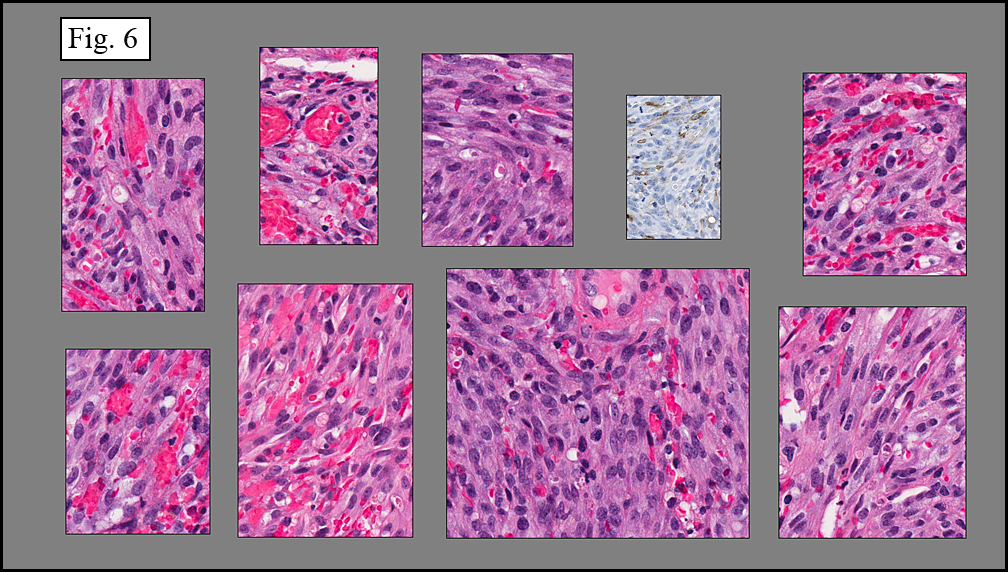
Microscopically the normal lymph node architecture was replaced by a disordered vascular proliferation (Fig. 2). The cells were spindled and showed a diffuse fascicular pattern (Fig. 3). Mitotic figures were increased (Fig. 4). Another characteristic was numerous slit-like spaces and regions containing many extravasated red blood cells (Fig. 5). Hyaline globules were also present (Fig. 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
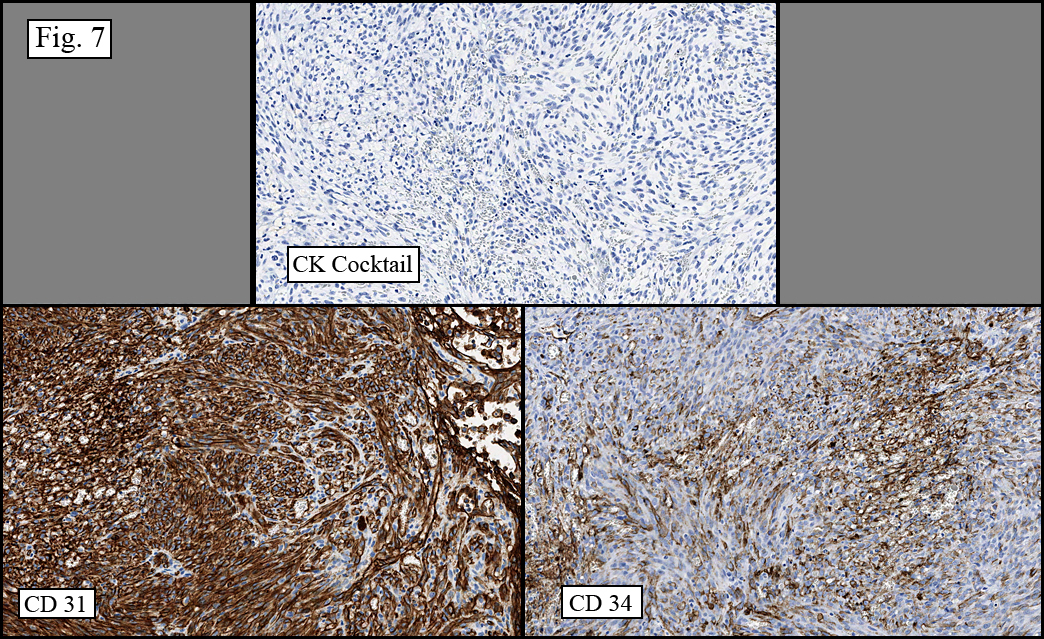
Immunostains for CD31 and CD34 were positive (Fig. 7). Markers for epithelial (Fig. 7), neural, melanocytic and lymphoid origins were negative.
{kind=link}
Diagnosis: “Kaposi Sarcomaâ€
Christina Martin MSIV, Donald R. Chase MD
Department of Pathology, Loma Linda University and Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Kaposi Sarcoma (KS) is a locally aggressive endothelial tumor that classically presents with blue-red nodular skin lesions which spread and coalesce into plaques. Lesions may also involve mucosal sites, lymph nodes, and visceral organs. KS is uniformly associated with human herpes virus 8 (HHV-8), and may arise in the context of immunosuppression. It is believed that HHV-8 establishes a latent infection in a number of cell types including B lymphocytes and endothelium, and that reactivation of latent virus is pivotal in the development of KS.
Four epidemiological forms are recognized:
1. Chronic (Classic) KS occurs predominantly in men (90%) during late adult life (peak incidence in 6th and 7th decades) of Mediterranean/Eastern European descent with the classic presentation of purplish, reddish-blue or dark brown plaques, macules, and/or nodules found most often involving the skin of the lower extremities. It is prevalent in certain parts of the world including Poland, Russia, Italy, and equatorial Africa, but rare in the United States, and shows a statistically significant association with a second malignant tumor or altered immune state. The disease is usually indolent with a prolonged clinical course.
2. Endemic (African) KS arises in children and adults in Equatorial Africa who are not HIV infected. It presents primarily as localized or generalized lymphadenopathy, with sparse skin lesions which tend to be truncal. The course of the disease is fulminant, a feature attributed to internal tumor involvement.
3. Iatrogenic KS (i.e. transplant-associated) is well-established in renal transplant patients. Incidence varies based on patient population, suggesting genetic susceptibility. It usually develops several months to a few years after transplant (average 16 months). The extent of the disease correlates directly with the loss of cellular immunity as measured by response to skin testing with phytohemagglutinin (PHA), conconavalin A (Con A), pokeweed mitogen (PWM), and dinitrochlorobenzene (DNCB). Clinical course improves with the patient’s ability to tolerate reduction in immunosuppression and worsens with organ or internal involvement.
4. Acquired immunodeficiency syndrome-associated KS (AIDS KS) occurs in the setting of immunodeficiency caused by HIV-1 infection, which potentiates tumor growth. This form disproportionately involves the male homosexual population with other risk groups including intravenous drug users, sex trade workers and hemophiliacs receiving factor VIII-enriched blood fractions. Presentation is usually in young adults with initially small, flat, pink patches on the skin which later progress to classic blue violet papules, with a predilection for lines of cleavage and mucosal surfaces. It may also metastasize or synchronously involve deep viscera/organs.
Treatment for KS in limited mucocutaneous disease usually consists of local therapy including cryotherapy, intralesional injections and radiation therapy. Mortality is 10-20%. In patients with AIDS, KS responds to highly active antiretroviral therapy (HAART). The mortality rate in AIDS KS has decreased from 90% to less than 50%. AIDS patients with KS, usually die of secondary (opportunistic) infections many times due to pulmonary compromise.
The KS phenotype may be found in other tumors, generally as a minor component:
• Well-differentiated angiosarcoma (AS) has features virtually indistinguishable from early KS skin lesions, however a careful history (lifestyle, immunosuppression, etc) is of great importance. KS also tends to be HHV-8 positive while AS is generally negative.
• Fibrosarcoma can be confused with the advanced lesions of KS. The presence of ectatic slit-like spaces and inflammatory cells at the periphery of the lesions, and hyaline globules point towards KS, as does positivity for HHV-8.
• Arteriovenous malformations may duplicate the skin lesions of KS and have been termed “pseudo KS†but lack the marked spindling and formation of slit-like lumens of KS. They may present with bruits or by touch, “thrillsâ€.
• Spindle-cell hemangioendothelioma (aka Kaposiform hemangioendothelioma) is often confused with KS. A younger population, without immunosuppression favors SCH, as does cavernous vessels and epithelioid endothelial cells. The preservation of lobules (not found in KS) is also helpful.
Suggested Reading:
Enzinger and Weiss’: Soft Tissue Tumors 5th Ed. Editors Weiss SW, Goldblum JB. Mosby, Inc. pp 722-730, 2008.
World Health Organization Classification of Tumours: Pathology & Genetics Tumours of Soft Tissue and Bone. Editors Fletcher CDM, Unni KK, Mertens F, pp 170-172, 2002.
An unusual cause of a parotid mass in an immunocompetent host: Classic Kaposi’s sarcoma. Pagani D, Bellinvia M, Capaccio P, Scoppio B, Brambilla L, Pignataro L. Tumori. 2009 Mar-Apr; 95(2);248-50.
Kaposi sarcoma in unusual locations. Pantanowitz L, Dezube BJ. BMC Cancer. 2008 Jul 7;8:190. Review.
Lymph nodes involved by multicentric Castleman disease among HIV-positive individuals are often involved by Kaposi sarcoma. Naresh KN, Rice AJ, Bower M. Am J Surg Pathol. 2008 Jul;32(7):1006-12.
Fine needle aspiration cytology determinants of the diagnosis of primary nodal Kaposi’s sarcoma as the first sign of unknown HIV infection: a case report. Morelli L, Pusiol T, Piscioli I, Del Nonno F, Brenna A, Licci S. Acta Cytol. 2007 July-Aug;51(4):602-4.