History: An otherwise healthy 44-year-old man presented with a three month history of a painless lump over his right hip. Aspiration of the mass was dry, yielding no fluid. Surgical excision was performed, finding a 4.0 cm, smooth, pink, slightly glistening soft tissue tumor just proximal to the greater trochanteric region. The tumor was solid, without hemorrhage or necrosis.
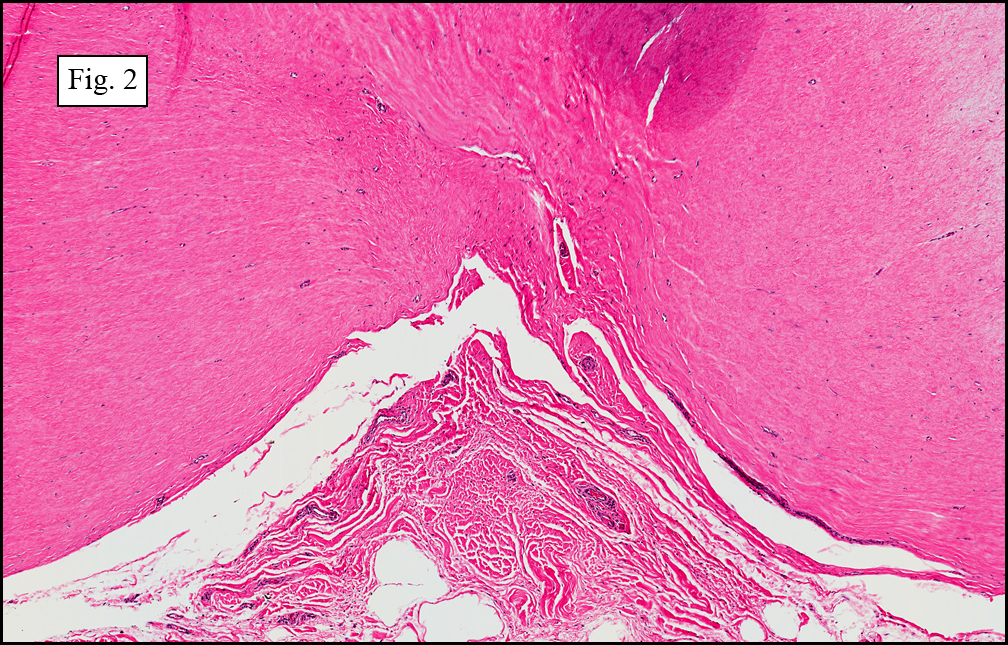
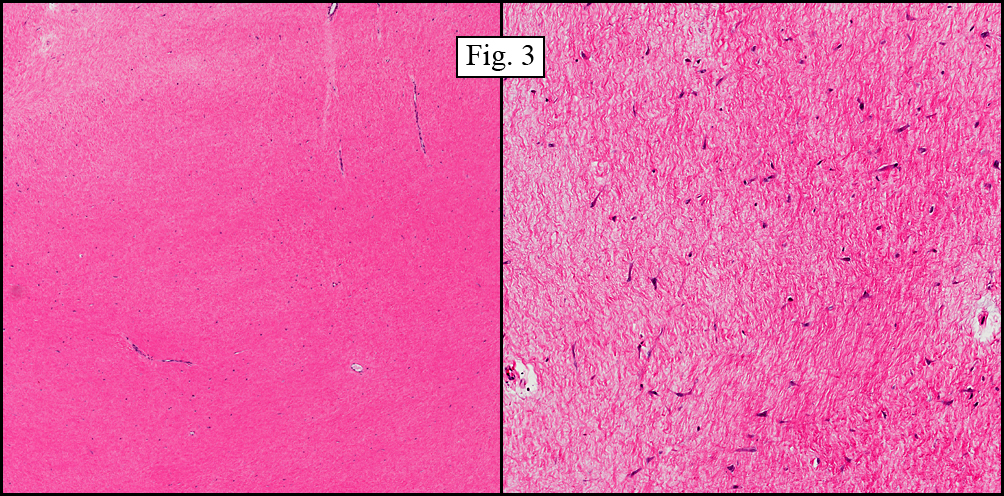
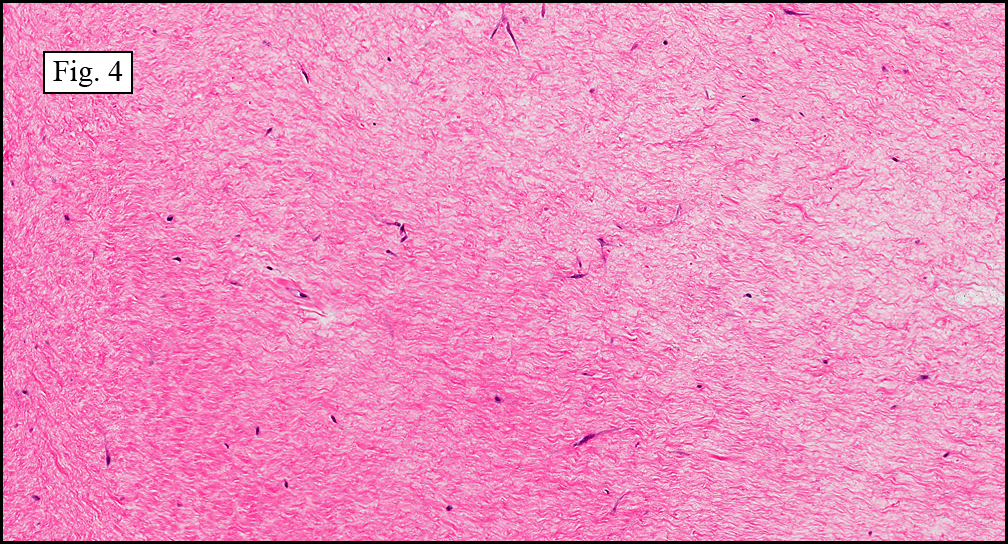
Microscopically, the mass was composed mostly of thick, hypocellular collagenous tissue (Fig. 1). It was well-circumbscribed and minimally associated with adjacent soft tissue (Fig. 2). Widely interspaced within the collagen were stellate to spindle-shaped cells resembling fibroblasts and myofibroblasts (Fig. 3, 4). The tumor lacked pleomorphism and did not display mitotic figures.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Desmoplastic fibroblastoma (Collagenous fibroma)
Miriam Peckham, PSF, and Donald R. Chase, MD
Department of Pathology and Human Anatomy, Loma Linda University and
Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Described first by Evans in 1995, desmoplastic fibroblastoma (DFB) is a rare, benign fibrous soft tissue mass that occurs most commonly in the skeletal muscle and subcutaneous tissue of adult males (5:1). This tumor presents most often in the fifth and sixth decades (mean 57 years) as a slow-growing, mobile, painless mass. The most common presentation sites include the upper and lower extremities, with the head and neck regions affected less frequently. The size of this tumor is normally less than 4 cm, but has been reported up to 20 cm.
Microscopically DFB is characterized by thick collagenous to myxocollagenous stroma with interspersed spindle and stellate-shaped fibroblasts/myofibroblasts. There are rare to absent mitotic figures and virtually no necrosis, hemorrhage or cellular atypia. Though DFB has the low-power appearance of a well-demarcated lesion, fat entrapment and infiltration of the surrounding soft tissues are commonly seen. Immunohisto- chemically, DFB positively marks for vimentin, and focally, expresses muscle-specific actin and alpha-smooth muscle actin. The tumor is generally negative for desmin, S-100 protein, and CD34.
Tumor behavior is usually indolent, with a slowly expanding soft tissue mass, which, when adequately excised, has limited capacity for local recurrence. To date, metastases have not been reported. This has led to question the nature of DFB and it has been reported that the tumor has a specific breakpoint at 11q12, supporting the notion that is a neoplastic process rather than a reactive one. Differential diagnoses include:
1. Nuchal fibroma: An uncommon lesion, nuchal fibroma most commonly occurs in the back of the neck of adult males. This lesion has a 30-40% association with diabetes and may recur after excision, most likely due to its persistent inciting cause. Histologically, its appearance is very similar to desmoplastic fibroblastoma in that it is made up of hypocellular collagen strands. Also seen are entrapped fat cells and an increased amount of small nerves. This morphology also overlaps with Gardner fibroma.
2. Gardner fibroma: Most commonly presenting in childhood, this lesion occurs mostly in the trunk with a predilection for the paraspinal region. The majority of patients with this lesion have familial adenomatous polyposis (FAP), with the fibroma preceding polyp formation. The correlation of this lesion with FAP makes the proper diagnosis of this fibroma of increased importance. These lesions are poorly demarcated and may recur as desmoid fibromatosis. Histologically, these fibromas show hypocellular collagen bands with artifactual cleft spaces. The cells within the mass have a bland, fibroblast-like appearance and there is frequently entrapment of surrounding soft tissue, all of which is similar to desmoplastic fibroblastoma. These masses stain positively for beta-catenin (similar as desmoid fibromatosis).
3. Neurofibroma: This lesion is characterized by wavy cells embedded within a myxocollagenous stroma. However, unlike desmoplastic fibroblastoma, they usually stain positive for S-100 protein.
4. Fibromatosis: This can be differentiated from desmoplastic fibroblastoma by its increased cellularity and its infiltrative nature. Another difference is this lesions characteristic cellular arrangement into broad fascicles.
5. Low-grade fibromyxoid sarcoma: This tumor is more cellular and more myxoid than DFB. It also tends to form whorls of spindled cells with a prominent fibromyxoid background.
6. Calcifying fibrous pseudotumor: This lesion affects a younger age group than DFB which is usually found in the fifth and sixth decades. This pseudotumor also shows a characteristic lymphoplasmacytic infiltrate, as well as multiple psammomatous calcifications located throughout its stroma.
7. Elastofibroma: This mass occurs mostly on the upper back in the region of the scapula. It is felt to be degenerative in nature, possibly due to repetitive motion. It diagnostically contains wavy elastic fibers which are absent in desmoplastic fibroblastoma.
8. Fibrous hyperplasia: Unlike desmoplastic fibroblastoma, this reparative inflammatory lesion presents with a history of trauma. The size of this lesion is also significantly smaller, ranging up to 1.5 cm.
9. Nodular fasciitis: This pseudosarcoma is more cellular, particularly in its early proliferative phase, and contains increased mitotic activity. It also shows rapid growth, contrasting with DFB which is indolent. A characteristic feature of NF is the mucinous separation of the tumor cells, resembling tissue paper that is being torn apart. The resolution stage of NF may mimic DFB, but is more cellular, mimicking benign fibrous histiocytoma.
Suggested Reading:
1. Watanabe H, Ishida Y, Nagashima K, Makino T, Norisugi O, Shimizu T. Desmoplastic fibroblastoma (collagenous fibroma). J Dermatol. 35(2):93-7, 2008.
2. Weiss SW, Goldblum JR. Soft Tissue Tumors, 5th Edition. Mosby Inc. through Elsevier Inc. Philadelphia. 2008.
3. Takahara M, Ichikawa R, Oda Y, Uchi H, Takeuchi S, Moroi Y, Kiryu H, Furue M. Desmoplastic fibroblastoma: a case presenting as a protruding nodule in the dermis. J Cutan Pathol. 35:70-3, 2008.
4. Walker KR, Bui-Mansfield LT, Gering SA, Ranlett RD. Collagenous fibroma (desmoplastic fibroblastoma) of the shoulder. AJR Am J Roentgenol. 183(6):1766, 2004.
5. Dagli M, Eryilmaz A, Acar A, Kulacoglu S, Akmansu H. Collagenous fibroma (desmoplastic fibroblastoma). Yonsei Med J. 45(5):941-3, 2004.
6. Shimoyama T, Horie N, Ide F. Collagenous fibroma (desmoplastic fibroblastoma): a new case originating in the palate. Dentomaxillofac Radiol. 34(2):117-9, 2005.
7. Fletcher, CDM. Diagnostic Histopathology of Tumors, 3rd Edition. Elsevier Limited. Philadelphia. 2007.