 History: A three-month old male presented for evaluation of an enlarging lesion on the right arm that had been present since birth. His mother noted rapid growth over the period of one month with central crusting of the lesion and minimal bleeding. The boy had been born full-term in a normal spontaneous vaginal delivery to a gravida 1, para 1 mother. He had no other medical problems and family history was noncontributory.
History: A three-month old male presented for evaluation of an enlarging lesion on the right arm that had been present since birth. His mother noted rapid growth over the period of one month with central crusting of the lesion and minimal bleeding. The boy had been born full-term in a normal spontaneous vaginal delivery to a gravida 1, para 1 mother. He had no other medical problems and family history was noncontributory.
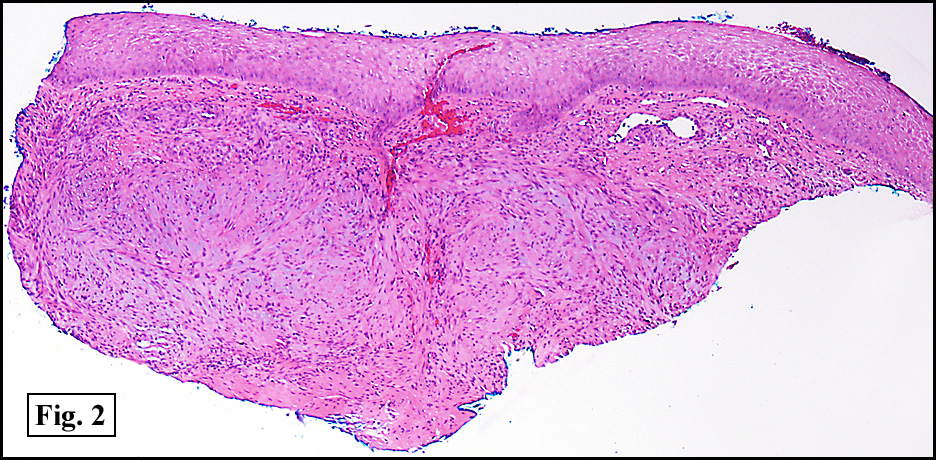
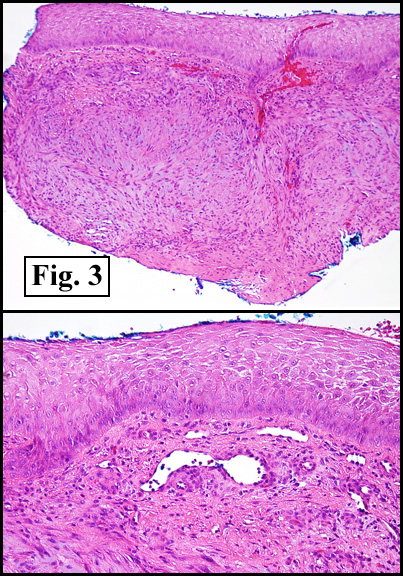
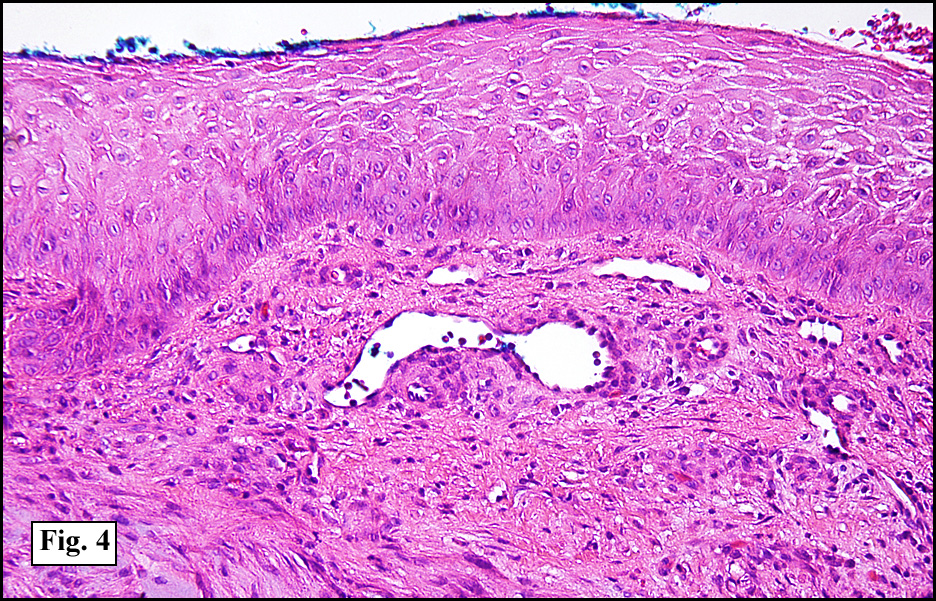
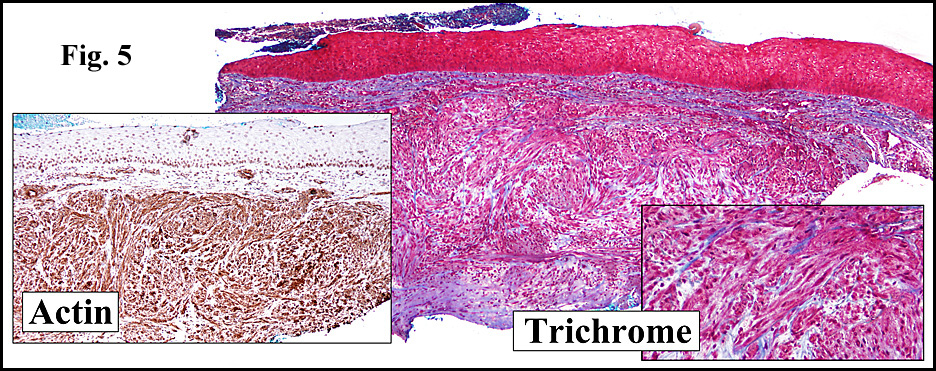
Physical examination revealed a 3.0 x 2.5 cm, well circumscribed nodule on an erythematous base with superficial crusting and ulceration (Fig. 1). The lesion was non-tender, firm, rubbery, and freely mobile. A 4-mm punch biopsy specimen was obtained (Fig. 2). It showed whorls and fascicles of smooth muscle as well as spindle-shaped myofibroblastic cells in a fibrous stroma (Fig. 3). Additional round to oval-shaped cells were present with surrounding vascular channels resembling a hemangiopericytoma pattern (Fig. 4). A trichrome stain highlighted muscular characteristics and an actin stain showed strong positivity (Fig. 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: “Solitary Congenital Infantile Myofibroma/Myopericytomaâ€
Tanya Nino; Katrina Woodhall, MD; Donald R. Chase, MD; Fred Soeprono, MD
Loma Linda University, California.
Department of Pathology and Human Anatomy,
Loma Linda University and Medical Center, Loma Linda, CA
California Tumor Tissue Registry, Loma Linda, CA
Discussion: Infantile myofibromatosis (IMF) was first recognized as a condition of benign fibrous spindle cell tumors in 1954 and was originally termed congenital fibromatosis. It was further classified in 1981 by Enzinger and Chung who recognized its myofibroblastic characteristics. Most recently IMF has been shown to be clinicopathologically connected to infantile hemangiopericytoma and it is thought that these tumors comprise a spectrum of the same entity. This condition must be considered in any neonate presenting with one or more skin or soft tissue tumors, as it is the most common juvenile fibrous tumor. It is divided into three forms:
1. solitary (>50% of cases)
2. multicentric superficial (>33%), and
3. multicentric with visceral involvement (<15%).
Clinically, IMF presents as one or more rubbery, firm, rounded nodules in the dermis or subcutaneous tissue. Superficial nodules may be mobile, yet it is not uncommon for deeper lesions to be fixed. The overlying skin is occasionally involved particularly with rapidly growing tumors and may show ulceration, crusting, ischemic necrosis, and purple or red discoloration. Lesions range from 0.5 – 7 cm in diameter and are non-tender. Approximately one-third of solitary lesions occur on the head, one-third on the trunk, with the remaining third on the upper or lower extremities. Bony involvement occurs approximately 50% of the time in the form of lytic metaphyseal lesions. Visceral tumors can involve the lungs, kidneys, heart, gastrointestinal tract, and even central nervous system. Female infants are more likely to have visceral involvement while males more often present with solitary lesions. Ninety percent of tumors appear within the first year of life.
Tumors of the solitary and multicentric forms follow a benign clinical course and often undergo spontaneous involution via rapid apoptosis within one to two years. However, some solitary tumors can grow rapidly, invading and destroying surrounding tissue. These more aggressive lesions may be treated with chemotherapy, allowing for shrinking of the tumor and alleviation of local tissue invasion. Visceral involvement confers a poor prognosis and is often fatal due to interference with the function of vital organs. Surgical intervention is only recommended for tumors causing obstructive or compressive symptoms. Although uncommon, IMF may recur later in childhood.
Suggested Reading:
- Baerg J, Murphy JJ, Magee JF. Fibromatoses: Clinical and pathological features suggestive of recurrence. J Pediatr Surg 34:1112-1114, 1999.
- Coffin CM, Dehner LP. Fibroblastic-myofibroblastic tumors in children and adolescents: a clinicopathologic study of 108 examples in 103 patients. Pediatr Patho 11:569-588, 1991.
- Chung, EB, Enzinger, FM. Infantile myofibromatosis. Cancer 48:1807-1818, 1981.
- Fletcher, CDM. Hemangiopericytoma, true pericytic tumors and mimics. United States and Canadian Academy of Pathology Meeting. San Diego, CA. March 25, 2007.
- Jurcic, V, Perkovic T, Pohar-Marinsek Z, Hvala A, Lazar I. Infantile myofibroma in a prematurely born twin. Pediatr Dermatol 20(4)345-349, 2003.
- Mentzel T, Dei Tos AP, Sapi Z, Kutzner H. Myopericytoma of skin and soft tissues: clincopathologic and immunohistochemical study of 54 cases. Am J Surg Pathol 30:104-113, 2006.
- Petit T, Grossin M, Fraitag S, Henin D. Solitary cutaneous infantile myofibromatosis. Ann Pathol 24(5):427-31, 2004.
- Wyatt AJ, Hansen RC. Pediatric skin tumors. Pediatr Clin North Am 47(4):937-963, 2000.