 History: A 53 year old woman presented with acute abdominal pain assumed to be diverticulitis. A right hemicolectomy was performed.
History: A 53 year old woman presented with acute abdominal pain assumed to be diverticulitis. A right hemicolectomy was performed.
The resected colon showed extensive serosal fibrinopurulent exudate. There was also an 8 x 7 x 4 cm mass in the cecum and ascending colon which narrowed the lumen by approximately 70%. It ulcerated the overlying mucosal and perforated into the underlying fat. The attached portion of ileum was uninvolved.
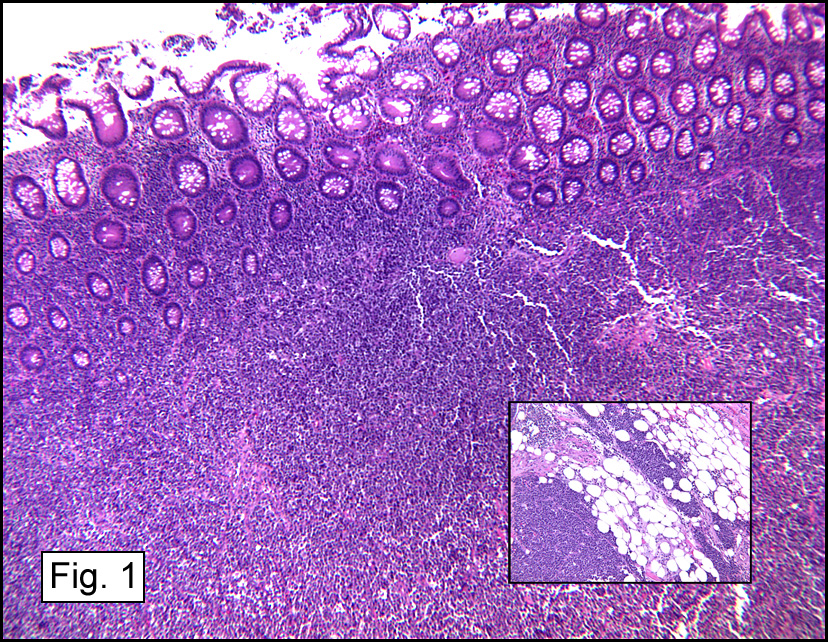
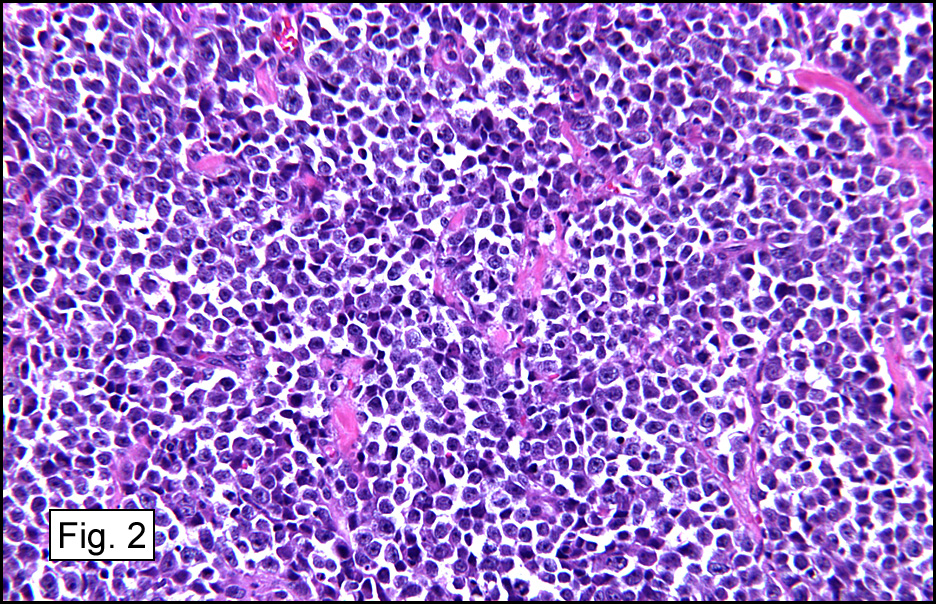
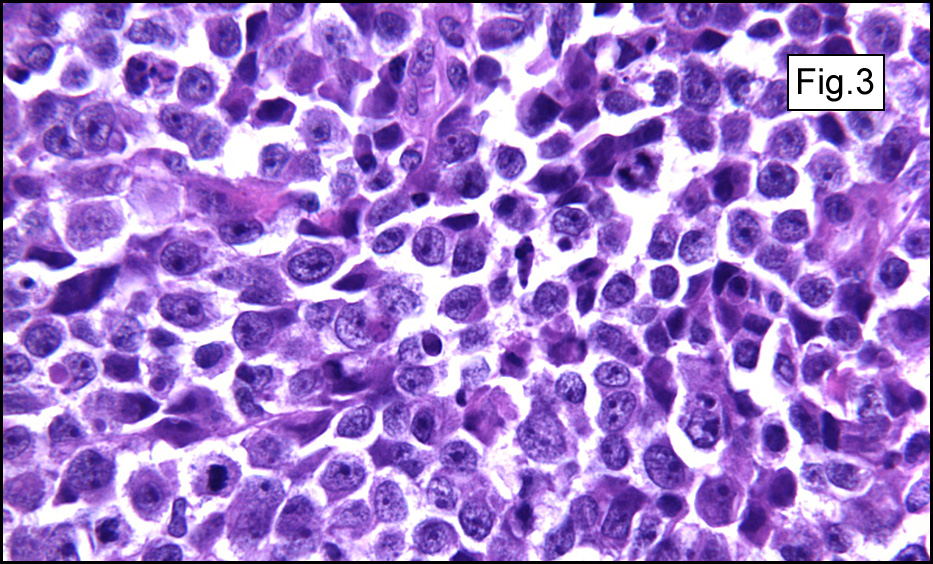
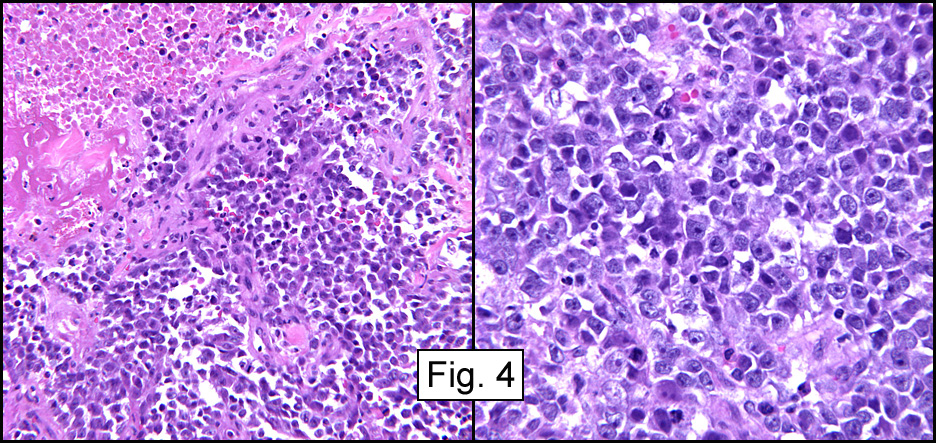
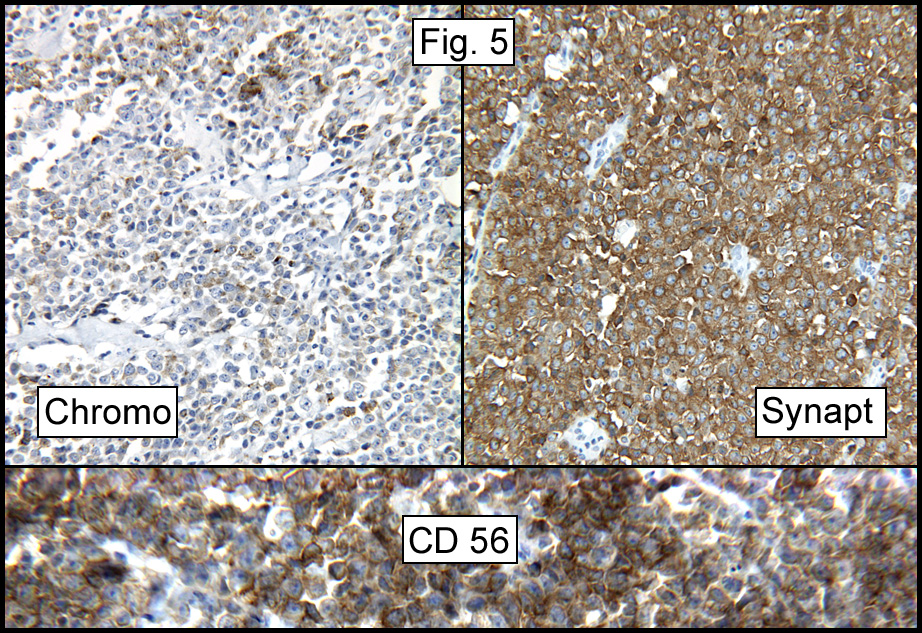
Microscopically, the tumor involved the submucosa with upward extension into the mucosa and more deeply into the muscularis and serosa (Fig. 1). The tumor was composed of sheets of fairly uniform large cells with a faint organoid growth pattern (Fig. 2). The cells were round to oval with moderate amounts of cytoplasm, vesicular nuclei and prominent nucleoli (Fig. 3). Numerous mitotic figures (up to 30/10 HPFs) were accompanied by apoptotic bodies as well as large areas of necrosis (Fig. 4). Immunohistochemically, the tumor cells were strongly positive for synaptophysin and CD56 and moderately positive for chromogranin (Fig. 5). They were negative for cytokeratins, CDX2, TTF1, CD45 and CD117.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Large Cell Neuroendocrine Carcinoma of the Cecum
Yvonne Noronha MD, Donald R Chase, MD
Department of Pathology and Human Anatomy,
Loma Linda University and Medical Center, Loma Linda, CA
California Tumor Tissue Registry, Loma Linda, CA.
Discussion: Originally described in the lung, large cell neuroendocrine carcinoma (LCNEC) has subsequently been reported in other organs. Because of its rarity, clear-cut criteria were originally lacking and the tumor was graded as if it was of pulmonary origin. But it is now recognized that unlike carcinoid tumors/atypical carcinoids, LCNEC is high grade, supported by their high mitotic rates, generally >10/10 HPF and aggressive clinical behavior.
Recently, in a study of 65 high grade neuroendocrine carcinomas of the GI tract, Shia et al used the WHO/ International Association for the Study of Lung Cancer criteria for pulmonary neuroendocrine tumors as a guideline to classify neuroendocrine carcinoma of the GI tract. To be classified as high grade neuroendocrine carcinoma, the tumor had to have >10 mitoses/10 HPF and had to fulfill criteria from one of the following three sub-groups:
1) Small cell carcinoma:
• Tumors with typical small cell morphology: markedly high nuclear to cytoplasmic ratio, hyperchromatic nuclei, finely granular chromatin with absent or faint nucleoli and frequent nuclear molding.
• Immunohistochemical evidence of epithelial differentiation: Positive staining for AE1:AE3.
• Positive staining for neuroendocrine markers helps but was not a requirement for diagnosis.
2) Large cell neuroendocrine carcinoma:
• Tumor with large cell neuroendocrine morphology: diffuse growth pattern/ neuroendocrine architecture (organoid growth pattern, trabeculae, and rosette formation); monotonous round to oval cells with moderate amounts of cytoplasm, granular or vesicular nuclei, with or without prominent nucleoli. Focal intracytoplasmic mucin or lumen formations were not criteria for exclusion.
• Positive immunohistochemical staining for chromogranin or synaptophysin in > 20% of tumor cells.
3) Mixed neuroendocrine carcinoma:
• Tumors showing histologic features in between small and large cell neuroendocrine carcinoma with immunohistochemical evidence of neuroendocrine differentiation.
The differential diagnosis of LCNEC is broad and should include (apart from carcinoids and small cell neuroendocrine carcinomas) lymphomas, plasma cell myelomas, poorly differentiated carcinomas and sarcomas. The correct diagnosis is based on the recognition of the typical morphology on H&E staining and is supported by the use of a limited immunohistochemical panel (synaptophysin and chromogranin). CD56 can be used but may not clarify the diagnosis since it can be positive with lymphomas, plasma cell myelomas, synovial sarcomas and rhabdomyosarcomas which are part of the differential diagnoses of LCNEC on H&E.
LCNECs are aggressive tumors. In one study of 83 cases of LCNEC of lung, the median survival was 17 months. The clinical significance of these tumors has yet to be fully evaluated. Their recognition, however, is of potential therapeutic significance since their neuroendocrine nature links them to classic small cell carcinomas which are sensitive to chemotherapy. Reports available to date regarding the chemosensitivity of LCNECs are contradictory. Although there are no prospectively controlled data, surgical resection when feasible, followed by combination chemotherapy similar to that employed for small cell carcinoma, appear to offer the best chance for improved survival in patients with early stage disease.
Suggested Reading:
1. Hamilton S.R and Aaltonen L.A. World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of the Digestive System. Lyon: IARC Press; 2000.
2. Travis WD, Colby TV, Shimosato Y, et al. in association with Sobin LH and pathologists from 14 other countries. WHO/IASLC Classification of Lung and Pleural Tumors. Berlin: Springer; 1999.
3. Shia J, Tang LH, Weiser MR et al. Is Nonsmall Cell Type High-Grade Neuroendocrine Carcinoma of the Tubular Gastrointestinal Tract a Distinct Disease Entity? Am J Surg Pathol 32(5): 719-731, 2008.
4. Bernick PE, Klimstra DS, Shia J et al. Neuroendocrine Carcinomas of the Colon and Rectum. Dis Colon Rectum 47: 163-169, 2004.
5. Gaffey MJ, Mills Se, Lack EE. Neuroendocrine Carcinoma of the Colon and Rectum. A clinicopathologic, ultrastructural and immunohistochemical study of 24 cases. Am J Surg Pathol; 14: 1010-1023, 1990.