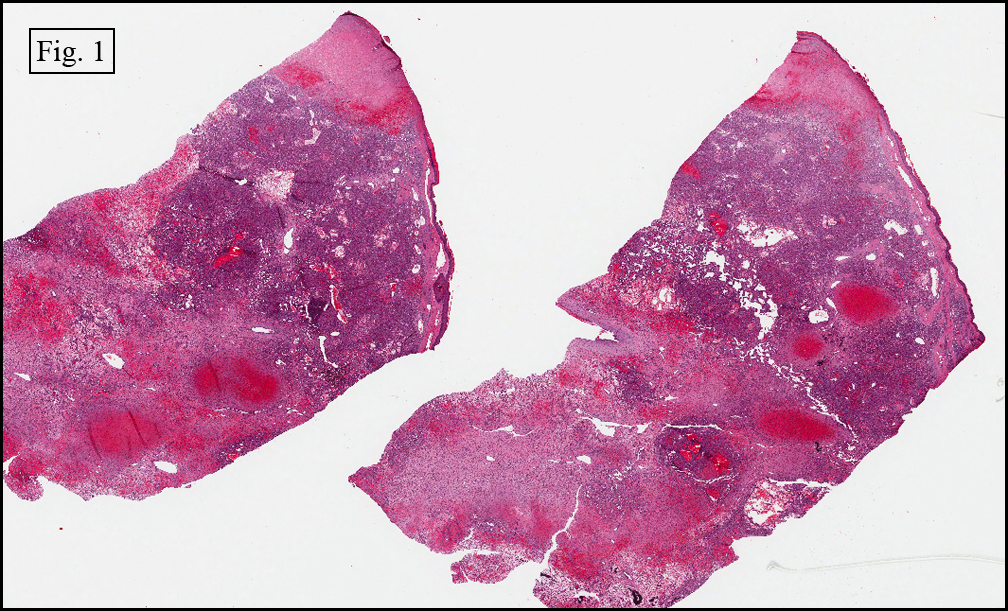
History: A three month old baby boy presented to plastic surgery clinic with a purple-red tumor on his right eyelid. Radiographs taken prior to surgery demonstrated a well-defined soft tissue mass without calcification.
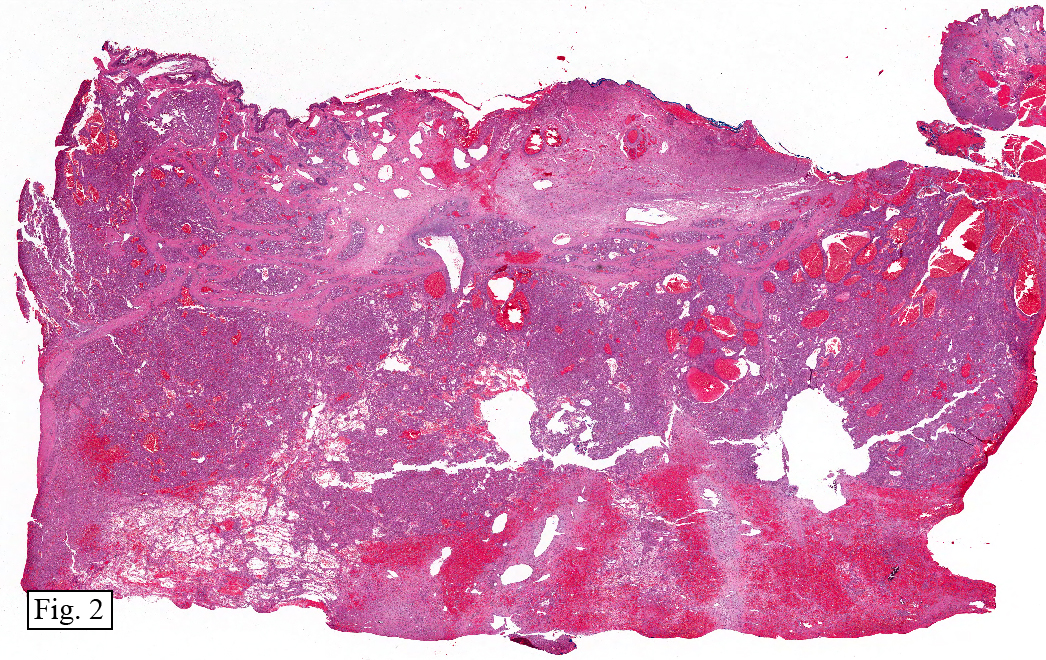
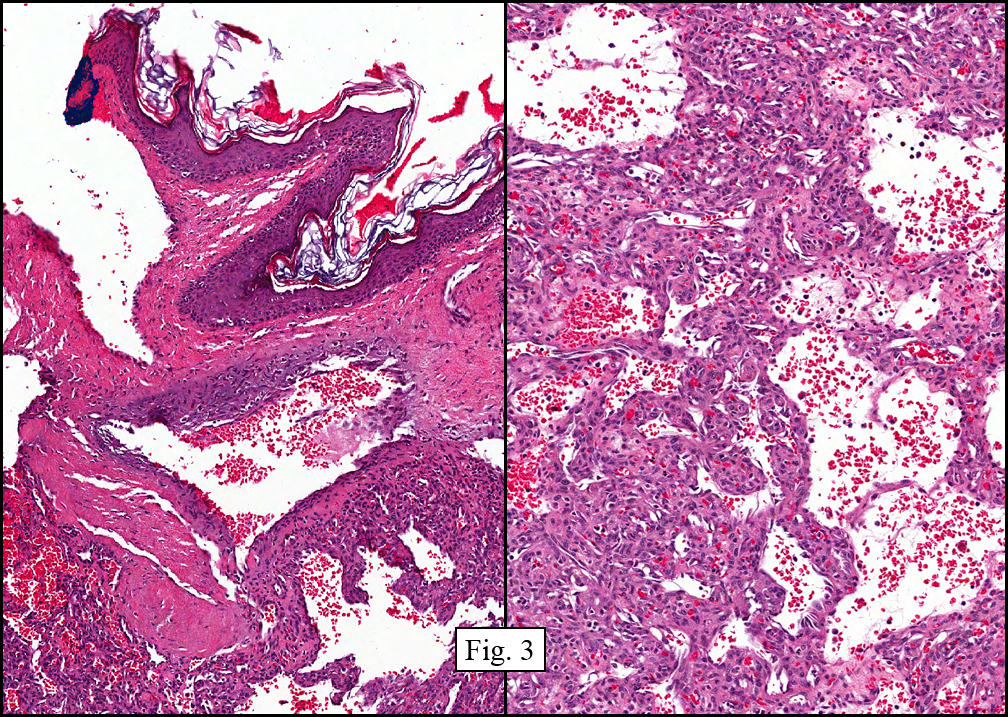
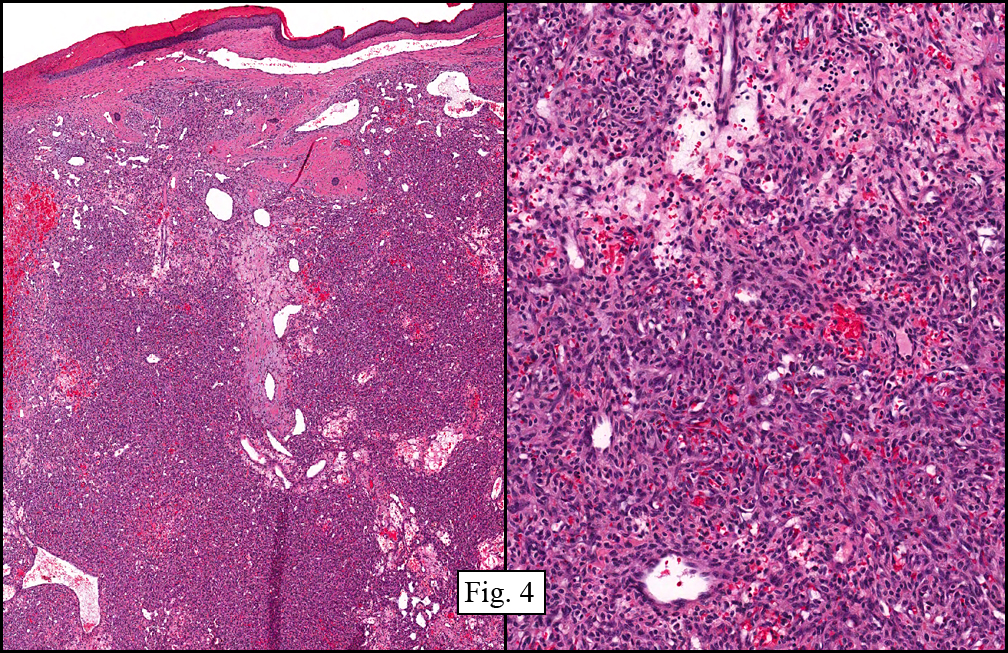
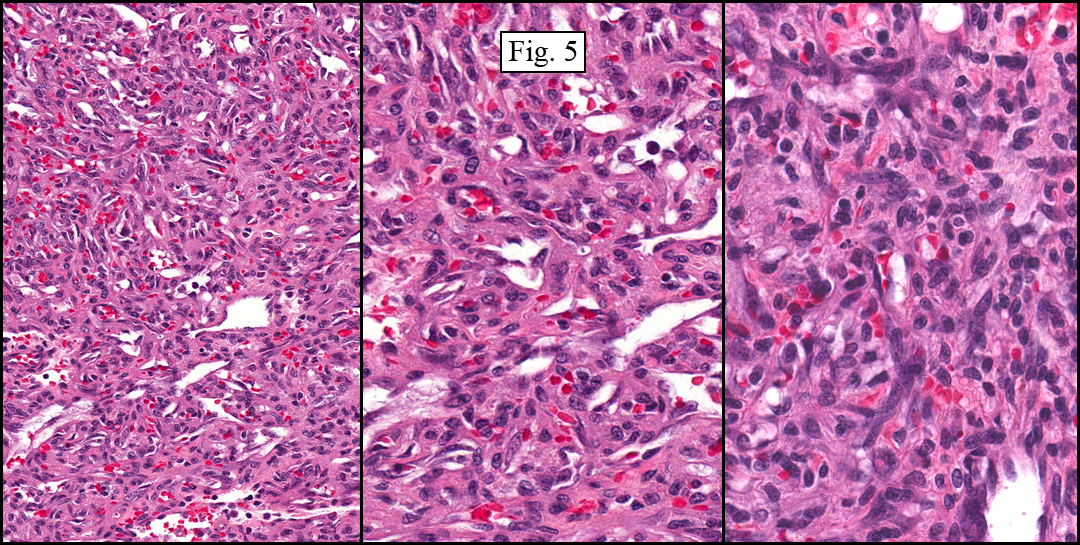
The resected specimen microscopically showed a mildly hyperkeratotic epidermis undermined by a cellular, vascular tumor (Fig. 1, 2). The tumor showed cyst-like spaces filled with blood, similar to changes seen in an aneurysmal bone cyst (Fig. 3). Much of the tumor was solid, supported by ectatic blood vessels, focally resembling a hemangiopericytoma vascular pattern (Fig. 4). Closer evaluation of the cells showed a striking resemblance to pericytes, and smaller, ectatic vascular spaces which were sometimes slit-like (Fig. 5). Mitotic figures were rarely encountered, and no significant cellular pleomorphism was seen. Immunostains confirmed the vascular nature of the tumor and were also positive for GLUT-1 (see reference).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis: Kaposiform Hemangioendothelioma of the Eyelid
Michael J. Matus PSF, Mia Perez MD, Donald R. Chase MD
Department of Pathology and Human Anatomy, Loma Linda University and
Medical Center, Loma Linda, California
California Tumor Tissue Registry, Loma Linda, California
Discussion: Kaposiform hemangioendothelioma (KHE) is a rare vascular tumor which can be locally aggressive and is most often found in skin, deep soft tissue, and/or bone in infants and children. Rarely does it occur in adults.
The term kaposiform refers to a morphologic resemblance to Kaposi sarcoma and the designation hemangioendothelioma implies its uncertain biologic behavior felt to lie between that of hemangioma and angiosarcoma.
Although KHE is often locally extensive and aggressive, it has not been shown to metastasize. Despite this, death has resulted due to severe coagulopathy related to the neoplasm. This association, termed Kasabach-Merritt syndrome (KMS), was described by Dr. Haig Haigouni Kasabach and Dr. Krom Merritt in 1940. Also known as Hemangioma with thrombocytopenia this syndrome occurs when a vascular tumor traps platelets, resulting in severe thrombocytopenia and consumptive coagulopathy in which clotting factors are activated and fibrinogen is diminished, worsening the bleeding tendency. This progress can progress to disseminated intravascular coagulation and death.
The differential diagnosis of Kaposiform hemangioendothelioma includes:
1) Kaposi sarcoma
2) Infantile (juvenile) hemangioma
3) Congenital non-progressive hemangioma
4) Tufted angioma
Unlike EHE, Kaposi sarcoma rarely occurs in children (except for the African lymphadenopathic form) and is usually associated with human herpesvirus 8 (HHV8), a result not found in EHE. There are several different clinical presentations, however all bare the same microscopic pattern. Most commonly occurring in adults, a flat red to purple lesion signals early tumor involvement, mirrored by a histologic proliferation of miniature vessels surrounding central ecstatic vessels. As vascular proliferation continues, bland spindle cells appear on the periphery. These spindle cells, devoid of significant pleomorphism, coalesce into distinct nodules and are eventually separated by slit-like spaces that contain erythrocytes.
Infantile hemangioma is the most common vascular tumor of infancy and occurs in nearly 4% of children. Histologically, tumor lobules are separated by normal appearing stromal elements composed of fibroblasts, pericytes, mast cells, and in some cases interstitial dendritic cells. The endothelial cells are prominent, and often contain significant rough endoplasmic reticulum and, by electron microscopy, Weibel-Palade bodies. This vascular lesion is immunoreactive to CD31, CD34, factor-VIII-related antigen as well as GLUT1 (see reference).
Congenital non-progressive hemangioma differs from EHE by being fully formed at birth with subsequent involution in most cases. A peripheral rim of pallor with a central depressed ulcer vividly portrays this change if the involution is rapid. The histological distinction from EHE is that the tumor lobules are surrounded by dense connective tissue. Also the clinical appearance of the overlying skin is often atrophic and microscopically, it lacks adnexal structures.
The term Tufted angioma (TA) was coined in 1989 by Wilson-Jones and Orkin for a tumor previously termed angioblastoma. Grossly the lesion presents as pink macules and plaques that grow slowly then stabilize. Histologically, there is an abundance of angiomatous lobules along the periphery of the lesion with fewer in the central region. In addition, they often include eccrine glands and venules surrounded by dense connective tissue. This appearance closely mimics EHE, and some authorities include TA in the EHE category, splitting them only by age of presentation. EHE appears to be the juvenile form, and TA, the adult form of what may actually be the same tumor. Both diagnoses are important, however, as each can give rise to Kasabach-Merritt syndrome, especially when deeply located in soft tissue or in the retroperitoneum.
The identification of EHE is important mostly for its association with KMS. Unlike congenital non-progressive hemangioma, it does not regress and therefore requires total surgical extirpation. To date, the separation of EHE from tufted angioma is mostly based upon patient age. Both, however, can give rise to KMS.
Suggested Reading:
Rastogi S, Banerjee S, et al. Glut-1 antibodies induce growth arrest and apoptosis in human cell lines. Cancer Letters, 253(2):244-251, 2007.
Lai, FMM, To, KF, Choi PCL, Leung PC, Kumta SM, Yuen PPM, Lam WY, Cheung ANY, Allen PW. Kaposiform Hemangioendothelioma: Five Patients with Cutaneous Lesion and Long Follow-Up. Mod Pathol 14(11):1087-1092, 2001.
Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 69:412-422, 1982.
North PE, Waner M, Beckmiller L, James CA, Mihm Jr MC. Vascular tumors of infancy and childhood: beyond capillary hemangioma. Cardiovascular Pathology 15:303-317, 2006.
North PE, Waner M, James CA, Mizeracki A, Frieden IJ, Mihm Jr MC. Congenital Nonprogressive Hemangioma. Arch Dermatol 137:1607-1620, 2001.
Weiss, SW, Goldblum, JR. Enzinger & Weiss’s Soft Tissue Tumors. 5th Ed. Mosby Inc.
Wed, Jul 21, 2010
Added missing author, Dr. Perez